









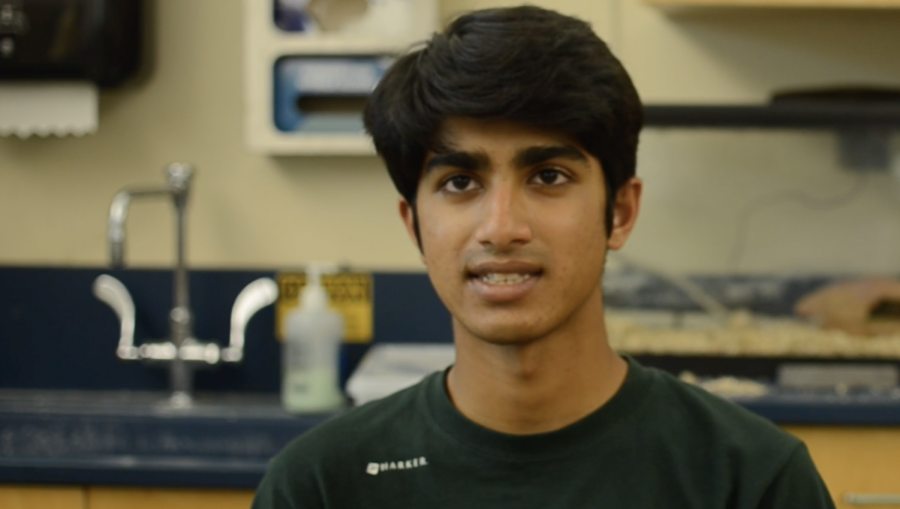
![“[Building nerf blasters] became this outlet of creativity for me that hasn't been matched by anything else. The process [of] making a build complete to your desire is such a painstakingly difficult process, but I've had to learn from [the skills needed from] soldering to proper painting. There's so many different options for everything, if you think about it, it exists. The best part is [that] if it doesn't exist, you can build it yourself," Ishaan Parate said.](https://harkeraquila.com/wp-content/uploads/2022/08/DSC_8149-900x604.jpg)



![“When I came into high school, I was ready to be a follower. But DECA was a game changer for me. It helped me overcome my fear of public speaking, and it's played such a major role in who I've become today. To be able to successfully lead a chapter of 150 students, an officer team and be one of the upperclassmen I once really admired is something I'm [really] proud of,” Anvitha Tummala ('21) said.](https://harkeraquila.com/wp-content/uploads/2021/07/Screen-Shot-2021-07-25-at-9.50.05-AM-900x594.png)




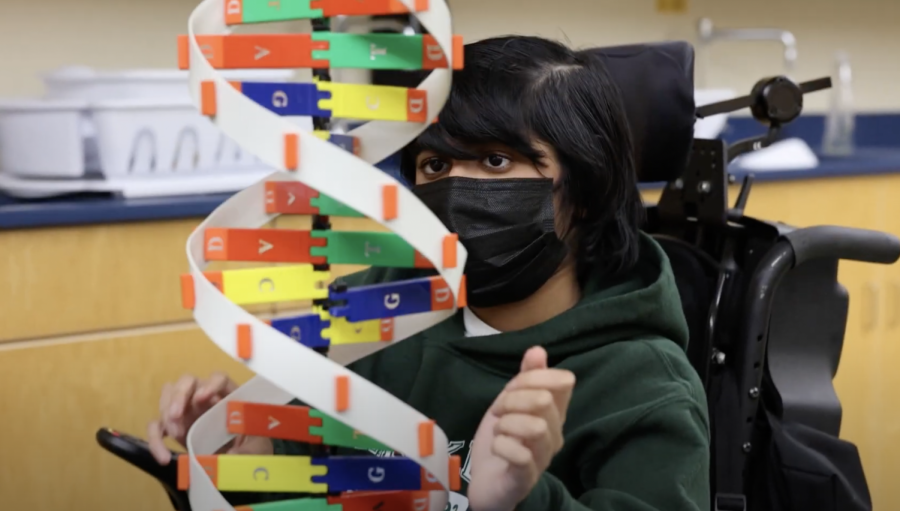
![“I think getting up in the morning and having a sense of purpose [is exciting]. I think without a certain amount of drive, life is kind of obsolete and mundane, and I think having that every single day is what makes each day unique and kind of makes life exciting,” Neymika Jain (12) said.](https://harkeraquila.com/wp-content/uploads/2017/06/Screen-Shot-2017-06-03-at-4.54.16-PM.png)








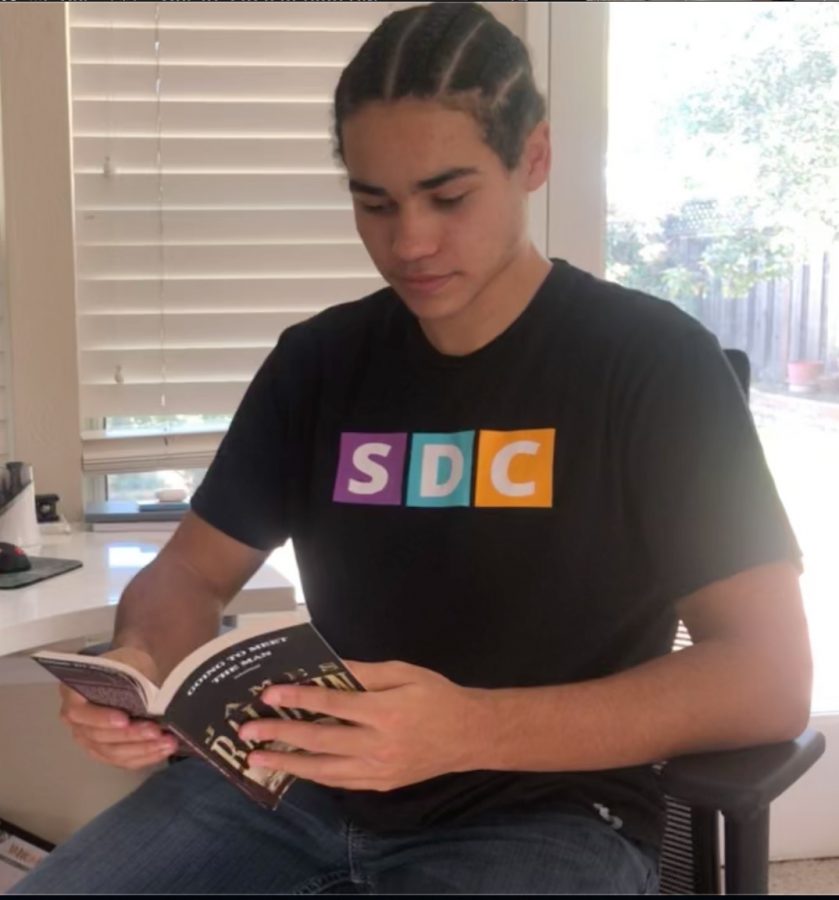
![“My slogan is ‘slow feet, don’t eat, and I’m hungry.’ You need to run fast to get where you are–you aren't going to get those championships if you aren't fast,” Angel Cervantes (12) said. “I want to do well in school on my tests and in track and win championships for my team. I live by that, [and] I can do that anywhere: in the classroom or on the field.”](https://harkeraquila.com/wp-content/uploads/2018/06/DSC5146-900x601.jpg)
![“[Volleyball has] taught me how to fall correctly, and another thing it taught is that you don’t have to be the best at something to be good at it. If you just hit the ball in a smart way, then it still scores points and you’re good at it. You could be a background player and still make a much bigger impact on the team than you would think,” Anya Gert (’20) said.](https://harkeraquila.com/wp-content/uploads/2020/06/AnnaGert_JinTuan_HoHPhotoEdited-600x900.jpeg)

![“I'm not nearly there yet, but [my confidence has] definitely been getting better since I was pretty shy and timid coming into Harker my freshman year. I know that there's a lot of people that are really confident in what they do, and I really admire them. Everyone's so driven and that has really pushed me to kind of try to find my own place in high school and be more confident,” Alyssa Huang (’20) said.](https://harkeraquila.com/wp-content/uploads/2020/06/AlyssaHuang_EmilyChen_HoHPhoto-900x749.jpeg)




Trigger warning for topics of sexual assault.
In discussions about military trauma, an oversimplified, distinct division is often made between combat trauma and sexual trauma, with the former usually associated with men and the latter with women. However, the reality is far more complex: combat and sexual trauma are not confined to gender expectations but are experiences that can shape any service member’s reality.
A national study by the Department of Veteran Affairs found that about one in three women and one in 50 men go through some form of military sexual trauma, showing how MST affects service members of all genders at an alarming rate. MST is defined by the VA as “any unwanted sexual contact, threatening sexual behavior or sexual harassment that occurs during military service.” It still remains in the shadows, underreported and unacknowledged by the military, despite impacting the psychological and physical health of numerous male and female service members.
History teacher Karen Haley, who served in the Army’s Adjutant General Branch, highlights the flawed institutional response to MST, emphasizing how reports are often mishandled by 05s (Lieutenant Colonels) and 06s (Colonels).
“The full bird colonel, if they’re an 05 or if they’re an 06, they don’t necessarily want MST on their watch,” Haley said. “They transfer you and magically give you new orders, so you go to a different military installation. There’s no therapy, no real follow through with any procedure and survivors suffer the rest of their life.”
Survivors often develop a myriad of symptoms of post-traumatic syndrome disorder or post-traumatic stress disorder, which include hypervigilance and difficulties with emotional regulation. The survivors have nowhere to lean for support because the very institution that is meant to protect them becomes the source of pain, compounding their sense of betrayal.
Carolyn Allard, a psychology professor at Alliant International University, MST researcher and clinical psychologist, explains how survivors experience betrayal trauma.
“One of the things that makes MST lead to worse outcomes for victims of trauma is the betrayal component,” Dr. Allard said. “There needs to be more appreciation within the military of how impactful it is for someone to perpetrate MST on a victim within a group. That causes cohesion problems because when you’re in the military, you’re so dependent on the group.”
This sense of betrayal not only makes it harder for survivors to trust others but also contributes to greater post-traumatic difficulties with long term effects like depression, substance abuse, anxiety disorders and higher risk of suicide. Even with these severe outcomes, many MST incidents, particularly those involving male survivors, go unreported due to stigma and fear of ostracization because of the military’s collectivized nature.
Treatments for MST range from evidence-based psychotherapies like cognitive processing therapy and prolonged exposure therapy to pharmacological interventions for managing symptoms of PTSD. Many survivors struggle to access proper MST treatment in a timely fashion due to the stigma associated with reporting MST. Dr. Allard points out initiation of treatment as one of the biggest difficulties victims face when dealing with MST.
“People who experience interpersonal trauma may have to try therapy many times before they stick to it,” Dr. Allard said. “I used to work in a military sexual trauma clinic, and sometimes, veterans in their seventies and eighties had never sought treatment for decades and lived with their post-traumatic distress.”
The lack of specialized MST clinics is a direct consequence of military leadership and policymakers failing to grasp the full scope of the crisis. Dr. Allard underscores the need for more focused care that acknowledges the distinct and severe nature of MST.
“Our hospital had the military sexual trauma and interpersonal trauma clinic, but when I left, they dissolved that,” Dr. Allard said. “All MST cases were sent to the PTSD Clinic or General B Med Clinic, which is somewhat helpful, but it’s really important for clinicians to be trained specifically to deal with issues that are specific to survivors of MST.”
Accurately measuring the prevalence of MST poses a significant challenge as well. The military’s questionnaire for measuring sexual harassment, the Sexual Harassment Core Measure (SHCore), has many flaws. The SHCore fails to capture the full scope of MST in a predominantly male institution because it was developed from the Sexual Experiences Questionnaire based on experiences of non-military college women. Furthermore, the SHCore requires a reading grade higher than 9.1 due to the dense verbiage of the questions asked, excluding the 10% of military personnel who did not finish high school.
Dr. Allard expands on how the phrasing of questions can contribute to institutional silencing and underreporting.
“If you ask outright, ‘Have you ever been raped or sexually assaulted?’ a lot of people don’t define what happened to them as that,” Dr. Allard said. “There are psychological reasons why humans don’t want to admit that that happened to us, especially when we’re still in the context of where it could happen. People in general are more likely to open up if they are asked something like, ‘Have you ever had unwanted touching?’”
Individuals who cannot fully comprehend the verbiage of the survey’s questions end up providing “satisficed” answers that appear valid but fail to convey an accurate or thoughtful representation of their experiences. This skews the data and downplays the sexual harassment individuals go through in reports that go to the military leadership.
There must be increased standardization and inclusivity in MST research in order to tackle the numerous barriers MST survivors face. Expanding the scope of measurements like the SHCore would ensure that studies account for demographic differences like gender and education level.
On the whole, the military’s approach to addressing MST and its surrounding culture must be improved. Dr. Allard emphasizes the need for a cultural shift driven by military leadership.
“Leadership really needs to set a different culture of that does not permit any form of misogyny, sexual orientation discrimination and sexual harassment or abuse,” Dr. Allard said. “It needs to come from the top. It needs to be very clear. It needs to be zero tolerance.”